

What is Trigeminal Neuralgia?
Trigeminal Neuralgia is a pain condition which is typically caused by pressure on the brain nerve (cranial nerve) that gives feeling to the side of the face. Signals travelling through this trigeminal nerve cause debilitating and life-altering shock-like facial pain that lasts from seconds to hours. Initial episodes may be mild, but these can worsen over time if left untreated.
Symptoms of Trigeminal Neuralgia
Pain from Trigeminal Neuralgia almost invariably affects only one side of the face and can cause one or more of the following :
- Episodes of severe, shooting or jabbing pain that may feel like an electric shock;
- Spontaneous attacks of pain or attacks triggered by touching the face, chewing, speaking or brushing teeth;
- Episodes of several attacks lasting days, weeks, or rarely months;
- A constant aching, burning feeling that may occur before it evolves into the spasm-like pain of Trigeminal Neuralgia;
- Pain in areas supplied by the trigeminal nerve, namely the cheek, jaw, teeth, gums, lips, or less often, the eye and forehead;
- Pain triggered by facial contact or activity (such as shaving, washing the face, eating, drinking and talking).
What causes Trigeminal Neuralgia?
An expert witness on trigeminal neuralgia may be called to explain the causes of this condition. The most common cause of Trigeminal Neuralgia is contact between a healthy blood vessel (artery or vein) and the trigeminal nerve. The pressure from the contact with the blood vessel causes the trigeminal nerve to malfunction and send signals to the face that are perceived as pain. Other rare causes of Trigeminal Neuralgia include pressure from a benign tumor on the trigeminal nerve or damage to the nerve in patients with multiple sclerosis.
How is Trigeminal Neuralgia diagnosed?
A Trigeminal Neuralgia expert witness may assist the judge and or jury by describing how this condition is typically diagnosed. Diagnostic information includes the description of symptoms by the patient. Other rare causes can be ruled out through brain imaging.
How is Trigeminal Neuralgia treated?
 Treatment for Trigeminal Neuralgia starts with medication. First line medical therapy includes medications such as carbamazepine or oxcarbazepine. Many other medications can also be used including: baclofen, lamotrigine, levetiracetam, gabapentin, pregabalin, topiramate and botulinum injections. These medications vary in both their efficacy and tolerability.
Treatment for Trigeminal Neuralgia starts with medication. First line medical therapy includes medications such as carbamazepine or oxcarbazepine. Many other medications can also be used including: baclofen, lamotrigine, levetiracetam, gabapentin, pregabalin, topiramate and botulinum injections. These medications vary in both their efficacy and tolerability.
Treatment can progress to surgical intervention if the improvement from medication stops, or if the patient experiences unpleasant side effects from the drugs. The common types of surgery are microvascular decompression (MVD), radiofrequency lesion (RFL), and radiosurgery {gamma knife or LINAC-based).
How can Trigeminal Neuralgia be treated surgically?
A neurosurgeon expert witness on Trigeminal Neuralgia may also be asked to testify regarding surgical treatment options.
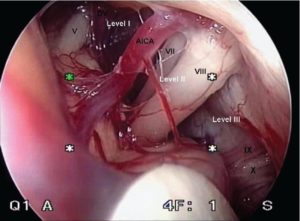 Microvascular Decompression (MVD) is a microsurgical neurosurgery that involves relocating or removing blood vessels that are in contact with the trigeminal root to stop the neve from malfunctioning. Decompression may reduce sensitivity and allow the trigeminal nerve to return to normal activity. MVD involves general anesthesia and making an incision behind the ear.
Microvascular Decompression (MVD) is a microsurgical neurosurgery that involves relocating or removing blood vessels that are in contact with the trigeminal root to stop the neve from malfunctioning. Decompression may reduce sensitivity and allow the trigeminal nerve to return to normal activity. MVD involves general anesthesia and making an incision behind the ear.
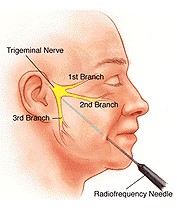 Radiofrequency Lesion (RFL). This does not require a breathing tube and general anesthesia. When performing an FRL, the neurosurgeon passes an approximately 3 inch long, pencil lead diameter, probe through the cheek until it arrives in the fibers of the trigeminal nerve. Those fibers are treated by numbing the part of the patient’s face which are experiencing pain. The procedure takes approximately 45 minutes and is done on an outpatient basis.
Radiofrequency Lesion (RFL). This does not require a breathing tube and general anesthesia. When performing an FRL, the neurosurgeon passes an approximately 3 inch long, pencil lead diameter, probe through the cheek until it arrives in the fibers of the trigeminal nerve. Those fibers are treated by numbing the part of the patient’s face which are experiencing pain. The procedure takes approximately 45 minutes and is done on an outpatient basis.
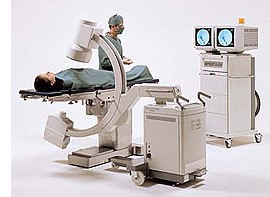

Brain stereotactic radiosurgery (Gamma knife) This treatment was developed in Europe. It begins with placement of a titanium, see-through box on the patient’s head. An MRI is followed by the patient lying on a table (see illustration) that moves the patient inside the treatment machine. The experience is very much like undergoing an MRI. The average treatment time is about an hour.
During this time, the treatment gamma knife machine focuses a large amount of radiation on the trigeminal nerve. The things people often associate with radiation such as fatigue, abnormal blood counts, hair loss, and nausea, only rarely occur. The box (frame) is removed, and the patient is usually home for lunch. In general, anything the patient did the day before treatment, the patient can do the day after.
Stephen C. Saris, MD is a board-certified neurosurgeon who practices in both Rhode Island and Massachusetts. His practice involves both brain and spine. Dr. Saris trained at Duke and Harvard. He is on the faculty of both Harvard and Brown. Dr. Saris is a highly experiences expert witness who has given more than 500 depositions and appeared in court more than 50 times. Office: (401) 453-3545 Fax: (401) 453-3533 Cell: (401) 378-2921 Email: ssaris@bwh.harvard.edu Web URL: www.neurosurgery-associates.com


