

By Jonathan Hersch, MD
Introduction
Over the last 20 years Orthopedics has moved towards a more minimally invasive way to perform the same procedures as we did open, such as rotator cuff repairs and ligament repairs of the shoulder. We have used a camera instead of a large incision to look inside the shoulder joint and perform repairs identical to the open procedures. The presumption has been that not only is there less pain but lower complication rates via the less invasive technique. However complications still occur, although rare. These complications are no less potentially serious or devastating. (1). After complications, an Orthopedic expert witness may be called upon to opine on whether the standard of care has been met.
Complications can occur during different phases of the surgical procedure: preoperatively, intraoperatively or post operatively. Careful attention to surgical positioning, technique, knowledge of anatomy, attentive anesthesia as well as patient education all are involved in preventing these complications from arising.
PREOPERATIVE COMPLICATIONS
Choosing the right patient
Choosing the right patient for the right procedure is paramount to ensuring surgical success. Screening for medical co-morbidities and correcting abnormalities such as uncontrolled hypertension and diabetes is the responsibility of the surgical and medical team. It is extremely important to explain to patients what to expect after surgery. They must be willing to participate in the postoperative regimen, if not increased complications and failure can occur.
Positioning of the patient
Surgery starts with positioning of the patient. Arthroscopic shoulder surgery can be performed in either the beach chair position (sitting up) or the lateral decubitus position (lying on the side). Each position has unique challenges and complications. The beach chair position set up is extremely important in that the neck must be positioned in a neutral position to avoid cervical spine injury. While sitting up anesthesia must pay attention to blood pressure as stroke can occur with hypoperfusion (2). The neck, arms and legs need to be well padded and protected, as nerve injury can occur during the surgery due to malposition and abnormal nerve pressure.

Beach Chair Position
Image courtesy Arthrex.com
The lateral position can cause nerve injury to the brachial plexus on the opposite shoulder as it lies under the patient. While performing arthroscopy, the surgical arm is placed in traction to open up the joint. The amount of weight is important to control as well as the position of the arm in traction. The down leg needs to be well padded to protect the peroneal nerve, which is superficial on the outside of the leg. Luckily most nerve injuries are neurapraxias, which are a low grade injury that resolve on its own. Longer surgeries can however lead to more severe, permanent injuries.

Lateral Position
Image courtesy Arthrex.com

Dr Hersch performing surgery with patient in lateral position
INTRAOPERATIVE COMPLICATIONS
Arthroscopic portals made around the shoulder are made with knowledge of the surface anatomy and the location of major nerves around the shoulder. As the surgery becomes more complex i.e. rotator cuff repair or labrum repairs, more and more portals need to be made to access different parts of the joint. The axillary, suprascapular and musculocutanoeus nerves are most at risk during surgery.
Axillary Nerve
The axillary nerve, which supplies motor function to the deltoid and teres minor muscles, can be vulnerable to injury by low, medial placement of the anterior portal of the shoulder. In addition procedures on the inferior capsule of the joint such as capsular release for frozen shoulder and stabilization for dislocations can cause injury to the axillary nerve. (3)
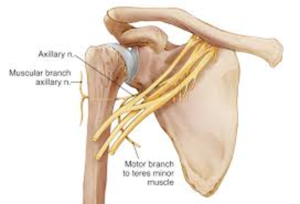
Image courtesy https://pathologies.lexmedicus.com.au/collection/axillary-nerve-injury
Suprascapular Nerve
The suprascapular nerve, which supplies motor function to the supraspinatus and infraspinatus muscles (rotator cuff), is vulnerable, when a retracted rotator cuff tear is released and pulled over to repair, stretching the nerve. Decompression of cysts around the nerve can also cause severe injury including complete transection. It is not a nerve easily visible and, if approached through a scope, knowledge of the anatomy is paramount
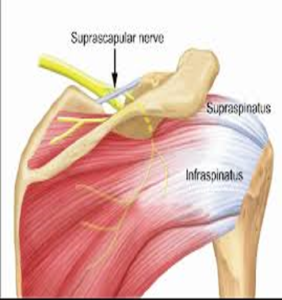
Image courtesy www.Raynersmale.com
Musculocutaneous Nerve
The musculocutaneous nerve, which supplies motor function to the biceps, brachialis and coracobrachialis muscles is particularly at risk during advanced procedures such as arthroscopic laterjet procedures for chronic dislocating shoulders. Placing multiple portals in the front of the shoulder also places this nerve in jeopardy.
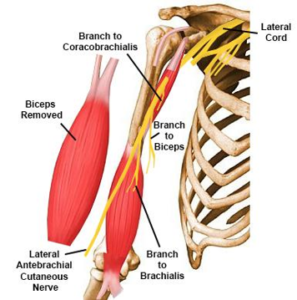
Image courtesy of www.orthobullets.com
POSTOPERATIVE COMPLICATION: Infection
Deep infection following arthroscopic shoulder surgery is a rare complication. If not treated upon detection it can lead to multiple surgeries, failure of the original surgery and chronic complications. Common risk factors for an infection are diabetes, obesity, smoking, peripheral vascular disease, previous surgery and recent steroid injection into the surgical joint. The rate of post op infection ranges from 0-3.4% in the literature (4)
How can we prevent infection? Some of these risk factors are controllable and some are not. Making sure all medical conditions are optimized before surgery is important. It is important to use the appropriate peri-operative dose of antibiotic. The skin preps used to clean the skin have been studied, and there are those such as chloraprep that are superior to others to diminish the normal presence of bacteria on the skin. (5)
One of the biggest problems with infections in shoulders in particular is the difficulty sometimes in recognizing it is there, making treatment delayed into the later stages of the infection. Symptoms sometimes are only pain or limited range motion while other common signs of infection such as redness and drainage of pus, are absent. Close follow-up with shoulder patients is key to picking up the signs of possible infection. Once suspected, treatment should be quick to identify the cause and treat with possible repeat surgery and antibiotics, which can be long term for deeper infections. Unfortunately infection can cause failure of previous surgery such as rotator cuff tears that “fall apart” when a deep infection arises. Repeat repair may need to be delayed until the infection is resolved and sometimes not possible due to breakdown of tissue leaving the patient with a chronic possibly unsolvable injury.
Conclusion
As with all surgeries, there is a level of risk that must be accepted by patient and physician. Complications can arise, even if in minimally invasive procedures such as shoulder arthroscopy. Attention to detail, proper patient selection and detection of complications when they arise are all part of keeping patients safe and on their way to full recovery. There are accepted standards of care practices to prevent major injury. When major injury does occur, Orthopedic surgeon expert witnesses may be called to opine whether the standard of care was met.
About the Author
Jonathan Hersch, MD is a board-certified orthopedic surgeon and expert witness,
who trained at the world famous Cleveland Clinic. He has extensive experience in
speaking/lecturing at national and international meetings. He can be reached at
jhersch1@gmail.com or 561-417-3339.
References
- Weber SC, Abrans JS, Nottage WM: Complications associated with arthroscopic shoulder surgery. Arthroscopy 2002; 18 (2, suppl1): 88-95
- Friedman DJ, Parnes NZ, Zimmer Z, Higggins LD, Warner JJ: Prevelance of cerebrovascular events during shoulder surgery and association with patient position. Orthopedics 2009;32(4):32
- Jerosch, J. Filler TJ, Peuker ET: Which joint position puts the axillary nerve at lowest risk when performing arthroscopic capsular relaease in patients with adhesive capsulitis of the shoulder? Knee Surg Sports Traumatol Arthrosc 2002; 10(2):126-129
- Randelli, P, Castagna A, Cabitza F, Cabitza P, Arrigoni P, Denti M:Infectious and thromboembolic complications of arthroscopic shoulder surgery. J Shoulder Elbow Surg 2010;19(1):97-101.
- Saltzman MD, Nuber GW, Gryzlo SM, Marecek GS, Koh JL: Efficacy of surgical preparationsolutions in shoulder surgery. J Bone Joint Surg Am 2009; 91(8):1949-1953.


